


Opioid Dependence vs Addiction Assessment Tool
What is this tool for?
Many people confuse physical dependence with addiction. This tool helps you understand the key differences based on symptoms and behaviors. Remember: physical dependence is a normal body response to opioids, while addiction (Opioid Use Disorder) is a brain disease.
This assessment is for educational purposes only and does not replace a professional diagnosis.
Physical Dependence Symptoms
Physical dependence occurs when your body adapts to opioids. Common withdrawal symptoms include:
Opioid Use Disorder (OUD) Symptoms
OUD is a brain disease with 11 diagnostic criteria. Check any of the following that apply:
Your Results
Many people think that if you take opioids for a while and then feel sick when you stop, you must be addicted. That’s not true. And this confusion is causing real harm - people are being denied pain relief, doctors are stopping helpful treatments, and patients are scared to take medication they actually need.
Let’s cut through the noise. Physical dependence and addiction are not the same thing. One is a normal body response. The other is a brain disease. Mixing them up leads to bad decisions - for patients, for doctors, and for public health.
What Physical Dependence Really Means
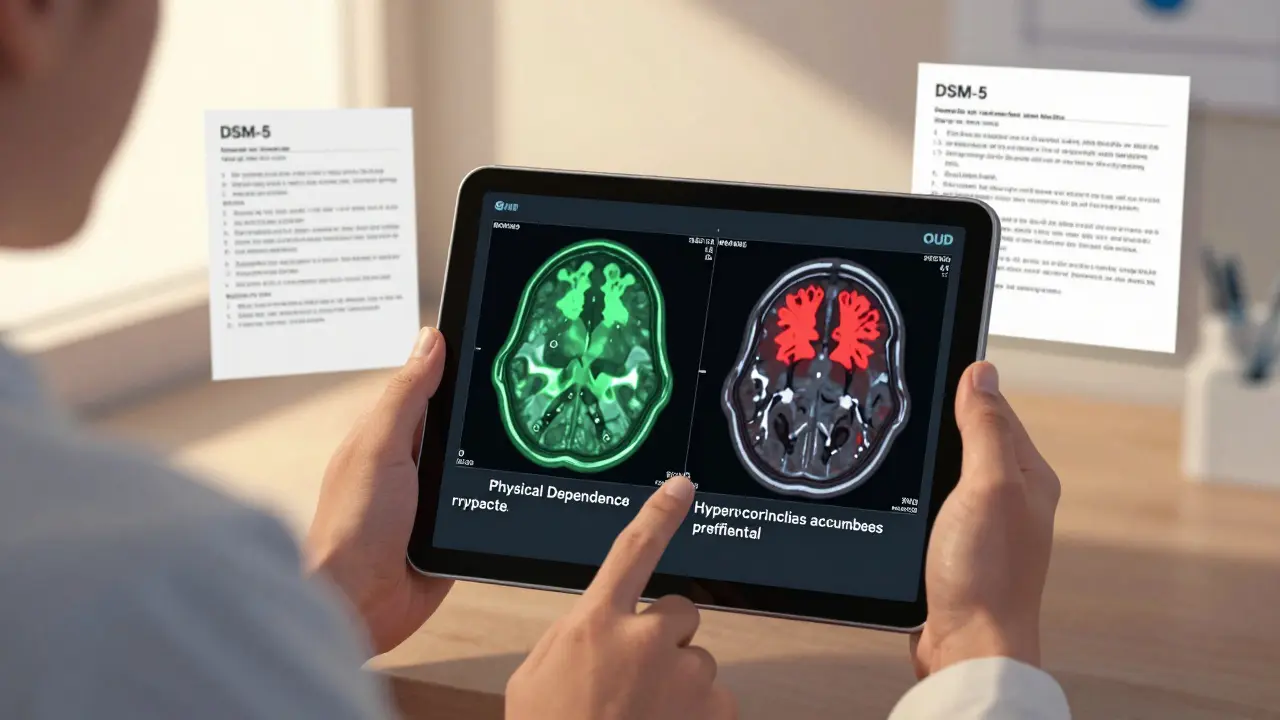
Physical dependence happens when your body adapts to having a drug in your system. It’s not about cravings or loss of control. It’s about chemistry. When you take opioids daily for more than a week or two, your brain changes how it works to compensate. Specifically, the locus ceruleus - a part of your brainstem that controls things like heart rate, sweating, and alertness - starts producing more norepinephrine to balance out the drug’s effects.
That’s why, when you stop taking the opioid, your body goes into overdrive. You get nausea, vomiting, sweating, anxiety, yawning, diarrhea - all the classic withdrawal signs. A 2003 study using the Clinical Opiate Withdrawal Scale (COWS) found that 92% of people experience nausea, 85% vomit, and 89% feel intense anxiety during withdrawal. These symptoms aren’t random. They’re predictable. They’re measurable. And they happen to nearly everyone who takes opioids regularly at doses above 30 morphine milligram equivalents (MME) per day.
Here’s the key: You can be physically dependent without being addicted. In fact, up to 100% of patients on long-term opioid therapy for chronic pain develop physical dependence. That doesn’t mean they’re using the drug illegally. It doesn’t mean they’re chasing highs. It just means their body got used to the medication.
What Addiction (Opioid Use Disorder) Actually Is
Addiction - now called Opioid Use Disorder (OUD) in clinical terms - is a brain disorder. It’s not about how long you’ve been on the drug. It’s about what the drug does to your decision-making, reward system, and self-control.
The brain circuits involved are different. While physical dependence affects the locus ceruleus, OUD changes the mesolimbic dopamine pathway - the same system that lights up when you eat, have sex, or win money. Over time, opioids hijack this system. The nucleus accumbens, the brain’s pleasure center, starts requiring more and more of the drug just to feel normal. Meanwhile, the prefrontal cortex - the part that tells you to stop doing dumb things - loses function. Studies show up to a 30% drop in activity here during impulse control tasks in people with OUD.
The DSM-5 (the official diagnostic manual used by doctors) says you have OUD if you have at least two of 11 symptoms in a 12-month period. These include:
- Craving - intense urge to use (present in 83% of severe cases)
- Loss of control - using more than planned or for longer than intended
- Continuing use despite harm - keeping to take opioids even after losing your job, relationship, or health
- Failure to fulfill obligations - missing work, school, or family events because of drug use
- Tolerance - needing higher doses for the same effect
Crucially, tolerance and physical dependence can happen without OUD. But if you’re stealing money to buy pills, lying to doctors for refills, or driving hours just to get more - that’s OUD. That’s not dependence. That’s disease.
The Numbers Don’t Lie
In 2017, a study in Pain Medicine found that while almost everyone on long-term opioids becomes physically dependent, only about 8% develop OUD. That’s a huge gap. And it’s backed up by the 2017 National Survey on Drug Use and Health: 9.9 million Americans misused prescription painkillers, but only 1.7 million met the full criteria for OUD.
Even more telling: A 2021 study in Pain Medicine found that among opioid-naïve patients (people who’d never taken opioids before) after surgery, only 0.7% to 1% developed OUD - even though nearly all became physically dependent. That means: taking opioids as prescribed after surgery doesn’t make you an addict. But fear of addiction? That’s what’s stopping people from getting proper care.
And here’s the real cost of confusion: A 2020 study in the Journal of Pain Research found that 68% of chronic pain patients believed withdrawal symptoms meant they were addicted. So they quit cold turkey. Or refused to refill. Or avoided opioids altogether - even when they were the best option for their pain.
How Doctors Tell the Difference
It’s not guesswork. There are tools. The CDC recommends using the Opioid Risk Tool (ORT) at the start of treatment. It looks at family history, past substance use, mental health, and age to predict who’s at higher risk for OUD. About 24% of patients are flagged as high-risk.
For someone who’s physically dependent but not addicted, the goal is safe tapering. The CDC recommends reducing the dose by 5-10% every 2-4 weeks. For patients on high doses (over 100 MME/day), go slower - 5% per month. Withdrawal symptoms are managed with tools like the COWS scale. A score above 12 means moderate withdrawal and needs attention.
For someone with OUD, tapering alone won’t cut it. They need Medication-Assisted Treatment (MAT). Buprenorphine cuts death risk by 70-80%. Methadone reduces it by 50%. These aren’t just replacements - they’re treatments that stabilize brain chemistry while therapy rebuilds behavior. Behavioral therapy is non-negotiable. MAT + counseling is the gold standard.
Why This Distinction Matters
When doctors mistake dependence for addiction, patients suffer. A 2021 article in PMC (PMC8583742) warned that this confusion leads to "stigma, discontinuation of needed medications, undue surveillance, and inappropriate treatment." Imagine being in severe pain, taking your meds exactly as prescribed, and then your doctor suddenly cuts you off because you developed withdrawal symptoms. That’s not care - that’s abandonment.
The American Medical Association passed a resolution in 2021 specifically urging doctors to "distinguish between physical dependence and substance use disorder." The CDC’s 2022 Guideline says outright: "Physical dependence is not a reason to discontinue opioid therapy when benefits outweigh risks."
Meanwhile, patients with true OUD are being failed too. If you think dependence equals addiction, you might assume someone on high-dose opioids must be abusing them - even if they’re following every rule. That leads to missed diagnoses and delayed treatment.

What’s Changing Now
Science is catching up. In 2023, researchers used fMRI scans to measure brain activity during craving tasks. They found they could tell physical dependence from OUD with 89% accuracy by looking at prefrontal cortex activation. That’s huge. Within the next 3-5 years, this could become a standard diagnostic tool.
The FDA approved lofexidine extended-release in 2023 specifically to ease opioid withdrawal symptoms - a sign that we’re finally treating dependence as a medical issue, not a moral failing.
And the NIH’s HEAL Initiative has poured $1.8 billion into developing non-addictive pain treatments. That’s not just about stopping opioids - it’s about giving people better options so they don’t have to choose between pain and risk.
Bottom Line
Physical dependence? It’s a normal, temporary side effect of long-term opioid use. It doesn’t mean you’re addicted. It doesn’t mean you’re weak. It just means your body did what bodies do - adapted.
Addiction? That’s a medical disease. It’s not about willpower. It’s about brain changes that make stopping feel impossible - even when your life is falling apart.
If you’re on opioids for pain, don’t panic if you feel sick when you try to stop. Talk to your doctor. Get a taper plan. Don’t quit cold turkey. You’re not addicted.
If you’re using opioids to get high, or you’re lying, stealing, or losing jobs because of them - you need help. Not judgment. Not shame. Treatment. MAT works. Recovery is possible.
The difference isn’t subtle. It’s life-changing. And it’s time we stopped confusing one for the other.
Can you be physically dependent on opioids without being addicted?
Yes. Nearly everyone who takes opioids daily for more than 7-10 days becomes physically dependent. This means their body adapts and withdrawal symptoms occur if the drug is stopped. But addiction - or Opioid Use Disorder - requires compulsive use despite harm, loss of control, and cravings. Studies show over 90% of patients on long-term pain therapy develop dependence, but only about 8% develop OUD.
Does physical dependence mean I need to stop taking opioids?
No. Physical dependence alone is not a reason to stop opioid therapy. The CDC and other medical organizations state that if opioids are effectively managing your pain and the benefits outweigh the risks, you should continue taking them as prescribed. Withdrawal symptoms can be managed with a slow, medically supervised taper - usually 5-10% dose reduction every 2-4 weeks.
How do I know if I have Opioid Use Disorder?
Opioid Use Disorder (OUD) is diagnosed using the DSM-5 criteria. You need at least two of 11 symptoms within 12 months. Key signs include: strong cravings, using more than intended, failing to meet responsibilities, continuing use despite relationship or job loss, and spending excessive time getting or recovering from the drug. If you’re stealing money, lying to doctors, or driving long distances just to get pills, you likely have OUD. A trained clinician can assess this using standardized tools with 94% accuracy.
What’s the difference between tolerance and addiction?
Tolerance means you need a higher dose to get the same effect - often because your body adapted to the drug. It’s common with long-term opioid use and doesn’t mean you’re addicted. Addiction involves compulsive behavior despite negative consequences. You can be tolerant without being addicted. But if you’re using more than prescribed, hiding use, or risking your health to get more - that’s addiction.
Is medication-assisted treatment (MAT) just replacing one drug with another?
No. MAT - using buprenorphine or methadone - is evidence-based treatment for Opioid Use Disorder. Unlike illicit opioids, these medications stabilize brain chemistry without causing euphoria. They reduce cravings, prevent withdrawal, and allow people to rebuild their lives. Studies show buprenorphine cuts overdose death risk by 70-80%. MAT is not substitution - it’s recovery. Combined with counseling, it’s the most effective treatment available.





11 Comments
Physical dependence ≠ addiction. 🧠💊 This is SO important. I’ve seen too many patients get cut off abruptly because providers conflated withdrawal with misuse. The COWS scale data? 92% nausea? That’s not ‘addiction’-that’s physiology. We need to stop pathologizing adaptation. 🙏
It’s fascinating how the neurobiological distinction between dependence and OUD has been so systematically obscured by moral panic. The DSM-5’s operationalization of OUD-particularly the inclusion of ‘craving’ as a diagnostic criterion-is a masterstroke of clinical precision. One wonders why public discourse lags behind the literature by decades.
Wait… so you’re telling me the government, the CDC, and Big Pharma are all in cahoots to normalize opioid use under the guise of ‘medical necessity’? 🤔 And now they’re using fMRI scans to ‘prove’ dependence isn’t addiction? That’s just more mind-control tech disguised as science. The NIH’s $1.8B HEAL Initiative? That’s not research-it’s a cover for pushing synthetic opioids under the radar. I’ve seen the videos. They’re watching us. 📡👁️
Thank you for laying this out so clearly. It’s easy to fear what we don’t understand. But when we confuse body adaptation with moral failure, we hurt real people. I’ve worked with chronic pain patients for 15 years. The ones who taper slowly with support? They thrive. The ones who quit cold turkey out of fear? They suffer. This isn’t about drugs-it’s about dignity.
Let’s be honest: 8% OUD rate? That’s a statistically insignificant number when you consider the societal cost. Why are we even enabling this? The ‘physical dependence’ argument is just a euphemism for chemical slavery. If you need opioids daily to function, you’re not managing pain-you’re addicted. And yes, I’m calling it. No more soft-pedaling.
Well said. The CDC’s tapering guidelines are spot-on. 5-10% every 2-4 weeks. Simple. Safe. Effective. And MAT isn’t ‘replacing one drug’-it’s restoring brain function. Buprenorphine saves lives. Period. No shame. Just science.
OMG. THIS. IS. EVERYTHING. 🙌 I’ve been screaming this from the rooftops for years! Physical dependence is like getting a tan-you don’t stop going outside because you’re ‘addicted’ to sunlight. It’s biology! And MAT? It’s not substitution-it’s rehabilitation. I’ve seen people go from homeless to holding jobs because of buprenorphine. That’s not magic. That’s medicine. 🌟
Look, I get it. But let’s not sugarcoat it-this is just another way to normalize drug use. America’s opioid crisis didn’t happen because of ‘misunderstanding.’ It happened because we gave out pills like candy. Now you want us to believe dependence isn’t a red flag? That’s dangerous. And un-American.
What’s fascinating is how this mirrors the historical stigmatization of epilepsy, depression, and even diabetes. We once called them ‘weaknesses.’ Now we call them diseases. The brain is an organ. Addiction is a neurological disorder. Why do we still treat it like a character flaw? The real tragedy isn’t dependence-it’s our refusal to evolve.
Oh, so now we’re supposed to believe the ‘8% statistic’? That’s from a study funded by pharmaceutical lobbyists. And ‘fMRI scans prove it’? Please. Science is a tool of control. If you’re taking opioids long-term, you’re chemically dependent. Call it what it is: addiction. Stop gaslighting people into thinking they’re ‘just dependent.’ They’re not. They’re hooked.
Just… thank you. I’ve been on long-term opioids for fibromyalgia. When I tapered, I felt like a criminal. No one told me withdrawal was normal. I thought I was failing. This post? It’s the first time I felt seen. 🤍