


Secondary Hypogonadism is a medical condition where the testes produce normal amounts of testosterone but the signal from the brain - specifically the pituitary gland and hypothalamus - is weak or missing. When that signal falters, men experience the classic low‑testosterone symptoms despite having functional testicular tissue. Understanding why the signal breaks down and how everyday choices can keep it strong is the first step toward protecting hormone health.
Key Takeaways
- Secondary hypogonadism stems from a disrupted brain‑testes communication pathway, not from testicular failure.
- Obesity, chronic illness, stress, and certain medications are the biggest risk drivers.
- Regular strength training, adequate sleep, balanced micronutrients and weight management can prevent most cases.
- Screening involves blood tests for total testosterone, LH, and FSH; early detection avoids long‑term complications.
- Medical therapy (e.g., hormone replacement) works best when paired with lifestyle fixes.
What Is Secondary Hypogonadism?
To keep it simple, think of the endocrine system as a three‑part radio: the hypothalamus creates the broadcast, the pituitary amplifies the signal, and the testes are the speakers. In secondary hypogonadism the broadcast (often Gonadotropin‑releasing hormone, or GnRH) is weak, so the pituitary releases lower levels of Luteinizing hormone (LH) and Follicle‑stimulating hormone (FSH). Those hormones tell the testes to crank out testosterone. When the signal drops, testosterone levels fall even though the testicular cells - the Leydig cells - are still capable of producing the hormone.
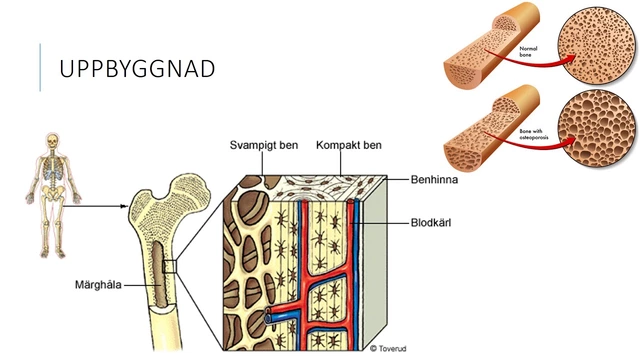
Typical signs mirror primary low‑testosterone: reduced libido, fatigue, loss of muscle mass, mood swings, and occasional bone density loss. The difference is the underlying cause, which means prevention focuses on brain‑centered health rather than solely on the testes.
Major Risk Factors to Watch
Not everyone who ages gets secondary hypogonadism, but certain conditions tip the scales. Below is a quick checklist of the most common culprits:
- Obesity - excess fat releases estrogen‑like compounds that feed back to the hypothalamus and suppress GnRH.
- Type 2 diabetes - insulin resistance interferes with hormone signaling pathways.
- Chronic inflammation - conditions like rheumatoid arthritis keep cytokines high, which dampen pituitary function.
- Opioid or glucocorticoid use - long‑term painkillers and steroids blunt GnRH release.
- Sleep apnea - fragmented sleep reduces nightly testosterone spikes and taxes the hypothalamic‑pituitary axis.
- Severe stress or depression - cortisol spikes compete with the reproductive axis for brain resources.
If any of these hit home, consider a proactive hormone check‑up before symptoms become noticeable.
Lifestyle Prevention Strategies
Think of these steps as maintenance for the brain‑testes radio. Each habit supports the hypothalamus, pituitary, or Leydig cells, keeping the signal strong.
1. Nutrition That Fuels Hormone Production
Focus on foods rich in zinc, vitamin D, and healthy fats - the building blocks of testosterone synthesis. Good sources include oysters, pumpkin seeds, fatty fish, and fortified dairy. Aim for 30‑45g of high‑quality protein per meal to sustain lean muscle, which in turn encourages healthy hormone balance.
2. Strength Training & High‑Intensity Interval Workouts
Resistance exercise spikes LH and FSH release, leading to a natural testosterone boost. A practical routine: three sessions per week, each containing 4‑5 compound lifts (squat, deadlift, bench press, rows, overhead press) performed for 3‑4 sets of 6‑8 reps. Add a 10‑minute HIIT finisher twice a week to amplify the hormonal response.
3. Prioritize Quality Sleep
Most testosterone is released during deep sleep (stage3). Target 7‑9hours of uninterrupted rest, keep the bedroom cool (≈68°F), and avoid screens at least an hour before bed. A short nap (<30minutes) on heavy‑training days can also help rebalance cortisol.
4. Manage Stress Effectively
Mind‑body practices such as meditation, breathing exercises, or even a daily 15‑minute walk lower cortisol, allowing the hypothalamus to focus on GnRH production. Consistency beats intensity - a brief daily habit is more beneficial than occasional long sessions.
5. Limit Alcohol & Avoid Smoking
Excess alcohol metabolizes into acetaldehyde, which interferes with testosterone synthesis. Limit intake to ≤2 drinks per week. Smoking introduces heavy metals that damage pituitary cells; quitting improves overall hormonal health within months.

When Medical Help Is Needed
If you notice any of the following, schedule a blood test with a primary‑care or endocrinology provider:
- Persistent low libido or erectile difficulty lasting >3months.
- Unexplained fatigue, depression, or loss of muscle strength.
- Significant weight gain despite stable diet and exercise.
The standard panel includes total testosterone, free testosterone, LH, FSH, and prolactin. Low LH/FSH alongside low testosterone points to secondary hypogonadism, whereas normal/high LH/FSH suggests primary testicular failure.
If labs confirm the diagnosis, doctors may discuss testosterone replacement therapy (TRT). While TRT can restore levels quickly, it does not address the root cause. Combining TRT with the lifestyle actions above yields the best long‑term outcomes and reduces the risk of side effects like erythrocytosis.
Comparison of Lifestyle vs. Medical Approaches
| Strategy | Effect on Testosterone | Typical Outcome Timeline | Key Considerations |
|---|---|---|---|
| Structured Strength Training + Nutrition | Up to +15% natural increase | 3‑6months of consistent effort | Requires discipline; benefits extend to cardiovascular health. |
| Weight Loss (≥10% body weight) | Can restore suppressed GnRH signaling | 6‑12months depending on baseline weight | Improves insulin sensitivity; may need professional guidance. |
| Testosterone Replacement Therapy (TRT) | Directly raises serum levels to target range | Within weeks after dosage adjustment | Cost, monitoring labs, potential side effects; does not fix underlying signal issue. |
The table shows that a well‑designed lifestyle plan often matches or exceeds the benefit of medication for mild‑to‑moderate cases, while TRT remains a powerful tool for more severe deficiencies.
Practical Daily Tips You Can Start Today
- Start each day with a protein‑rich breakfast (e.g., Greek yogurt + nuts) to jump‑start hormone production.
- Schedule three 45‑minute strength sessions per week; keep a log to track progressive overload.
- Drink a glass of water with a pinch of sea salt before workouts - sodium helps maintain blood pressure for optimal hormone delivery.
- Take a vitamin D supplement (1000-2000IU) if you live north of the 40° latitude or get <10minutes of sun daily.
- Set a bedtime alarm - “lights out” at the same time each night signals the hypothalamus to begin its nightly hormone cascade.
- Replace evening beer with a herbal tea (e.g., chamomile) to avoid alcohol‑induced testosterone dips.
- Use a stress‑reduction app for a 5‑minute breathing session before work meetings.
Stick with at least five of these for a month and re‑test your hormones. Most men see measurable improvement without any prescription.
Frequently Asked Questions
How is secondary hypogonadism different from primary hypogonadism?
Primary hypogonadism originates in the testes themselves - the Leydig cells can’t produce enough testosterone. Secondary hypogonadism starts higher up; the brain’s hypothalamus or pituitary fails to send the right signal, so the testes receive a weak cue despite being healthy.
Can losing weight reverse secondary hypogonadism?
Yes. Studies show that men who shed 10‑15% of body weight often see a 20‑30% rise in testosterone because excess fat’s estrogen‑like hormones drop, allowing the hypothalamus to resume normal GnRH secretion.
Do I need a specialist to get diagnosed?
A primary‑care doctor can order the initial hormone panel. If results point to secondary hypogonadism, they’ll refer you to an endocrinologist for deeper evaluation and tailored treatment.
Is testosterone replacement safe for a man with secondary hypogonadism?
When monitored correctly, TRT is safe and effective. However, it masks the underlying signaling issue, so doctors often combine it with weight loss, sleep optimization, or stress‑reduction programs to achieve lasting balance.
How often should I test my hormone levels?
If you’re in a prevention phase, an annual check‑up is sufficient. After starting any intervention-whether lifestyle or TRT-re‑test after 3‑6months to gauge response.
By keeping the brain‑testes communication line clear, you protect not just your libido but also bone health, muscle tone, and overall vitality. The good news? Most of the levers you need to pull are everyday choices you already control. Start small, stay consistent, and let your body do the rest.






16 Comments
Great summary! Keep it up.
Nice stuff! 😊
Yo, this is solid info. Just a heads up, make sure you grab enough zinc – like oysters or pumpkin seeds – they’re key for the hormone vibe.
You’ve got this.
Secondary hypogonadism is often portrayed as a mere side effect of aging, but the reality is far more intricate.
The hypothalamus, that tiny command center, can be silenced by a cascade of modern lifestyle choices.
Excessive sugary diets flood the bloodstream with insulin spikes that blunt GnRH release.
Chronic stress pumps cortisol to levels that outcompete the reproductive axis for neural resources.
Even a seemingly innocuous nightstand habit of scrolling through bright screens can sabotage the deep‑sleep hormone surge.
Obesity adds another layer of complexity, as adipose tissue converts testosterone into estrogen‑like compounds, feeding back negatively on the brain.
When the pituitary receives these mixed signals, it throttles LH and FSH secretion, leaving the testes idle despite their capacity.
The cascade is reversible, however, if we intervene with targeted nutrition, strength training, and sleep hygiene.
A diet rich in zinc, vitamin D, and omega‑3 fatty acids fuels the Leydig cells to stay ready for action.
Compound lifts such as squats and deadlifts provoke a natural spike in LH, essentially shouting to the pituitary to turn the volume up.
High‑intensity interval work adds a cardiovascular punch that further sensitizes the hormonal feedback loop.
Consistent weight loss of even ten percent can dismantle the estrogenic overload and restore GnRH pulsatility.
Medical therapy, while effective at raising serum testosterone, merely patches the antenna without fixing the transmitter.
Therefore, clinicians should prioritize lifestyle first, reserving hormone replacement for cases where the signal remains stubbornly muted.
Patients who combine TRT with disciplined exercise and nutrition often see better mood, strength, and metabolic outcomes than those who rely on pills alone.
In short, think of your endocrine system as a radio: keep the broadcast clear, amplify the signal, and the speakers will do their job without artificial interference.
While your enthusiasm is noted, let’s not overlook the shadowy influence of the pharmaceutical industry pushing testosterone gels as a quick fix. They profit from keeping the “signal” problem unsolved, steering patients toward lifelong prescriptions. A critical eye reveals that many of these products are marketed before rigorous long‑term safety data are available. Consider that the real power lies in reclaiming the body’s own broadcasting capability.
Enough with the half‑baked optimism! The real culprits are hidden agenda labs that flood us with endocrine disruptors. They lace processed foods with chemicals that deliberately mute GnRH, ensuring a captive market for their hormonal “solutions.” Wake up and cut the supply chain before you become a lab rat.
Just a heads up, many folks forget to check their vitamin D levels – a deficiency can really dampen the hypothalamic signal. A simple blood test can save a lot of future hassle.
Oh please, the “lifestyle miracle” narrative is just a glossy marketing ploy. You can’t outrun genetics with some kale smoothies and dumbbells – it’s a fantasy dressed up in rainbow hashtags.
While I respect your skepticism, the evidence does show that structured resistance training can improve LH pulsatility in many cases, even if genetics set a ceiling.
🔥💥This is the most EPIC guide EVER!💥🔥 I’m literally shouting from my balcony because your tips are 🔑 to unlocking the “inner god” vibe! 🏋️♀️💪🌟 Let’s all grab some oysters, smash a HIIT session and sleep like royal babies! 😴👑 #HormoneRevolution
The article provides a comprehensive overview of secondary hypogonadism, yet it could benefit from elucidating the specific neuroendocrine feedback mechanisms involved in GnRH pulsatility.
I’m curious about how chronic inflammation specifically interferes with pituitary LH secretion. Could anyone share recent studies that quantify this effect?
It is imperative to acknowledge that the singular focus on lifestyle modifications, while commendable, overlooks the substantial body of literature indicating that pharmacological intervention remains the most reliable method to restore eugonadal states in a timely manner. Randomized controlled trials have consistently demonstrated superior symptom amelioration with testosterone replacement therapy compared to exercise alone, especially in cohorts with pronounced LH deficits. Moreover, the variability inherent in dietary compliance and training adherence introduces confounding factors that diminish the reproducibility of purely non‑pharmacologic regimens. Consequently, clinicians ought to adopt a hybrid approach, privileging evidence‑based medication while concurrently encouraging ancillary lifestyle improvements. The notion that diet and strength training alone can fully re‑establish hypothalamic signaling is, at present, more aspirational than empirical.
Everyone, you’ve got the power to hit that reset button! Start with a protein‑rich breakfast, crush a solid squat session, and lock in 8 hours of deep sleep. Consistency is the secret sauce – keep grinding and you’ll watch your energy, mood, and confidence soar. Let’s crush those goals together! 💪🚀
Thank you all for the lively discussion – it’s clear that combining expert advice with personal experience creates the strongest strategy for tackling secondary hypogonadism. Wishing everyone health and balance.